The Story of Leonard Medical School at Shaw University
America’s First Four-Year Medical School and the Cradle of Black Physicians in the South
:
Tucked into the heart of downtown Raleigh, North Carolina, stands a twin-turreted brick building that most passersby walk by without a second glance. Yet behind its weathered Romanesque Revival walls lived a quiet revolution. Leonard Medical School at Shaw University was not just one of the earliest medical schools in America to train Black physicians — it was the first medical school of any kind in the United States to require a full four-year curriculum. For nearly four decades, it sent more than 400 Black doctors into the segregated South, often becoming the only physicians their communities had ever seen.
This is the story of how a Massachusetts missionary, a generous brother-in-law, and a class of six determined men changed American medicine forever.
Origins: A Mission Born of Necessity
The roots of Leonard Medical School reach back to 1865, the year the Civil War ended. That year, Reverend Henry Martin Tupper, a Baptist missionary from Massachusetts representing the American Baptist Home Mission Society, arrived in Raleigh determined to educate newly freed people. He founded what would become Shaw University, the oldest historically Black college in the American South.
It didn’t take Tupper long to notice another need. Between Washington, D.C., and New Orleans, there was not a single institution training Black physicians. African American communities across the South were medically abandoned, denied care by white doctors, and barred from white medical schools. Tupper began lobbying Shaw’s trustees for a medical department, framing it as a moral and practical necessity.
In 1880, the trustees agreed. Funding was cobbled together from the American Baptist Home Mission Society and a handful of Northern philanthropists. The single largest gift came from Tupper’s brother-in-law, Judson Wade Leonard, of Hampden, Massachusetts. In gratitude, the trustees named the new school in his honor.
Opening Day: November 1, 1881
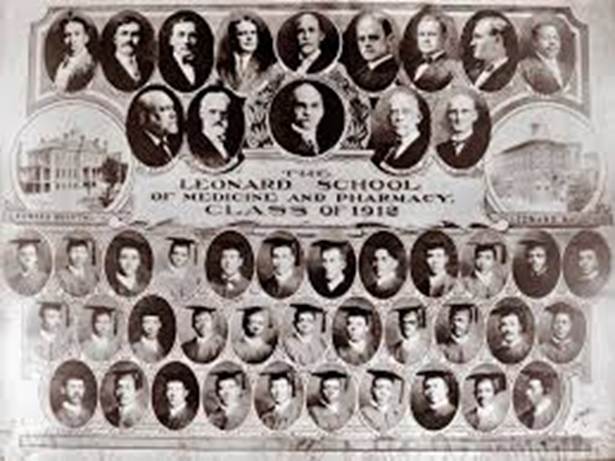
Construction of Leonard Hall began in the spring of 1881, with Shaw students themselves making the bricks to keep costs down. The building rose quickly, and on November 1, 1881, Leonard Medical School opened its doors with fifteen students and a tiny faculty of two.
Leonard Medical School, America’s first 4-year Medical School
By 1886, Leonard had quietly accomplished something no other American medical school Black or white had managed: a full, graded, four-year program. Most medical schools at the time required only two years of lectures, often repeated word-for-word in the second year. Leonard set a higher bar, and the rest of American medicine eventually followed.
Faculty of Leonard Medical School, ca. 1902.
The First Class: Six Men Who Made History
On March 31, 1886, Leonard Medical School graduated its first class — six men, every one of whom passed the state licensing board examination. Two were North Carolinians; the others came from Georgia, South Carolina, Virginia, and West Virginia. Class valedictorian Lawson Andrew Scruggs, born to enslaved parents in Bedford County, Virginia, would go on to become one of the first three board-certified Black physicians in North Carolina history. He served as resident physician at Leonard Hospital and later founded the Old North State Medical Society, the nation’s oldest professional association of Black physicians.
Among his classmates were Manassa Thomas Pope, who became a prominent Raleigh physician and ran for mayor in 1919, and J.T. Williams, who practiced in Charlotte, served twice on its Board of Aldermen, and was eventually appointed by President William McKinley as U.S. Ambassador to Sierra Leone, serving from 1898 to 1907. A middle school in Charlotte still bears his name.
The Instructors: An Unlikely Faculty
Leonard’s founding faculty consisted of just two men, both white Raleigh physicians. Dr. James McKee held the chair of physiology and medical principles and practice while continuing his own private practice across town. Dr. F.A. Spafford, already teaching classics at Shaw, took on the role of anatomy professor.
As enrollment grew, as many as 23 additional members of Raleigh’s white medical community served as part-time faculty across the school’s lifetime, a remarkable arrangement in the segregated post-Reconstruction South. Notable instructors included Kemp B. Battle Jr., son of the president of the University of North Carolina at Chapel Hill, and Wisconsin I. Royster, great-uncle of future Wall Street Journal editor Vermont C. Royster. Tuition was kept deliberately low, never more than $100 per year, roughly half what white medical schools charged and many students worked maintenance shifts in Leonard Hall itself to afford the rest.
Famous Graduates: From Raleigh to the World
If Leonard’s faculty was small, the legacy of its alumni was anything but. Perhaps the most celebrated graduate is Dr. Aaron McDuffie Moore, class of 1888. The son of free Black farmers in Columbus County, Moore completed Leonard’s four-year program in three years and ranked second among 46 candidates, 30 of them white, on the North Carolina medical board examination. He moved to Durham and became the city’s first Black physician.
Moore’s medical career was only the beginning. He co-founded the North Carolina Mutual Life Insurance Company in 1898, which grew into the largest Black-owned business in the United States. He persuaded tobacco baron Washington Duke to fund Lincoln Hospital, the first secular, freestanding hospital for African Americans in the state, instead of building a Confederate monument. He helped launch hundreds of Rosenwald schools for Black children across North Carolina, more than any other state in the nation. Today, Durham’s celebrated ‘Black Wall Street’ owes much of its existence to a Leonard graduate.
Dr. Aaron McDuffy Moore
Other notable alumni include Dr. Clinton Caldwell Boone (class of 1910), who served as a medical missionary in Liberia and the Belgian Congo, building schools, hospitals, and churches; Dr. John Walcott Kay (class of 1912), who co-founded the first hospital for African Americans in Wilmington, North Carolina; and Dr. George Louis Alphonso Pogue (class of 1911), who opened an integrated pharmacy in Bedford, Virginia, in 1912, a quietly radical act for the time.
The Closure: A Quiet, Devastating End
By the early 20th century, Leonard was struggling. Its endowment had always been modest, and most of its graduates served poor rural communities, leaving little capacity for alumni giving. Wealthier Black medical schools — Howard in Washington, D.C., and Meharry in Nashville — attracted the lion’s share of philanthropic dollars.
Then came the Flexner Report. Published in 1910 by Abraham Flexner under the Carnegie Foundation, the report was meant to standardize American medical education by tying schools to research universities and demanding modern laboratories, hospitals, and equipment. In theory, the goal was a uniform standard of care. In practice, the report was devastating for Black medical education. Flexner concluded that of the seven Black medical schools then operating, only two, Howard and Meharry, were ‘worth saving.’ Of Leonard, the report dismissively concluded the school ‘was in no position to make any contribution of value.’
Without resources to meet the new standards, Shaw’s trustees shortened Leonard’s curriculum to two years in 1914. The hospital closed that same year. The medical school held its final classes in 1918. By 1924, only Howard and Meharry remained among the nation’s Black medical schools, a loss the U.S. healthcare system has never fully recovered from.
The Legacy: Bricks, Bodies of Work, and a Building That Survived
In its 36 active years, Leonard Medical School graduated nearly 400 Black physicians — every one of whom passed state licensing examinations, an extraordinary record. They fanned out across the rural South, often as the only doctor for miles, delivering babies, treating tuberculosis, performing surgeries on kitchen tables, and quietly building a Black professional class that would help fuel the civil rights movement decades later.
Leonard Hall itself nearly didn’t survive. After the medical school closed, the building was repurposed for general classrooms. A 1986 fire destroyed its roof and left it derelict for over a decade. Then, in 2000, a $3.6 million grant from the Historically Black Colleges and Universities Fund combined with corporate donations brought it back. Today, Leonard Hall is a North Carolina Historic Landmark, a contributing structure in the East Raleigh-South Park Historic District on the National Register of Historic Places, and once again a working building on Shaw’s campus.
In 2006, the North Carolina Highway Historical Marker Program installed a plaque at the site. The marker is small. The story is enormous.
Leonard Medical School was a brief experiment in defiance, a place where freedom, faith, and science met for a few extraordinary decades. Its graduates carried that mission into the homes of patients who had been told their lives didn’t matter, and proved otherwise. The building that housed them still stands. So does the question its closure raises: how many lives were lost, and how much potential was stifled, when American medicine decided it could afford to lose schools like Leonard?
Galectin-3, Sepsis, and the Breakthrough Device That Could Change Critical Care Forever
A Web Blog Article | Science & Medical Innovation
Every two seconds, somewhere in the world, someone dies from sepsis. That is not a typo. Sepsis, a runaway inflammatory response to infection, kills more people each year than breast cancer, prostate cancer, and HIV combined. Yet most people have barely heard of it. What is even more remarkable is that for decades, scientists have been hunting for a single molecular villain at the heart of this catastrophe. They may have finally found it, a tiny protein called Galectin-3, and a new medical device is now being engineered to rip it right out of your blood.
This article takes you deep into the biochemistry, the clinical realities of sepsis, and the story of how one molecule became the focus of a potential revolution in critical care medicine.
What Is Sepsis And Why Should You Care?
Let’s start with definitions, because these terms are often used interchangeably but mean very different things:
Bacteremia is simply the presence of bacteria in the bloodstream. Think of it like a few unwanted guests slipping through the front door of your body. They are detectable but have not yet caused chaos.
Septicemia is an older, largely deprecated term that described active bacterial infection of the bloodstream, essentially bacteremia that had become a serious clinical illness.
Sepsis is something entirely different and far more dangerous. Sepsis is not the infection itself, it is your body’s own catastrophically dysregulated immune response to an infection. It is the fire your immune system lights to fight the enemy that burns your own house down.
Clinically, sepsis is diagnosed using a framework called the Sepsis-3 criteria, established in 2016. According to these criteria, sepsis occurs when an infection leads to life-threatening organ dysfunction, characterized by an increase of 2 or more points on the SOFA score (Sequential Organ Failure Assessment), which measures the failure of respiratory, coagulation, liver, cardiovascular, nervous, and renal systems.
The progression beyond sepsis is called septic shock, defined by the need for vasopressor medications to maintain blood pressure and elevated blood lactate levels, indicating the body’s cells are suffocating for energy.
Globally, sepsis is responsible for an estimated 11 million deaths per year, accounting for approximately 19% of all global deaths. In the United States alone, nearly 1.7 million adults develop sepsis annually, and roughly 270,000 die from it. The economic burden on the U.S. healthcare system exceeds $62 billion per year.
Who or What Causes Sepsis?
Sepsis is not caused by one pathogen. It can be triggered by a shockingly broad array of microorganisms:
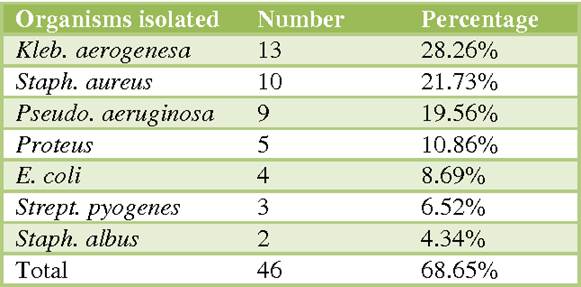
Common bacterial culprits include Escherichia coli (E. coli), Staphylococcus aureus (including the dreaded antibiotic-resistant MRSA), Streptococcus pneumoniae, Klebsiella pneumoniae, and Pseudomonas aeruginosa. These are the usual suspects, organisms well-known to emergency physicians and ICU teams.
Less common but equally dangerous are organisms like Listeria monocytogenes, Neisseria meningitidis (meningococcus), Clostridium species, Acinetobacter baumannii, and Enterococcus faecalis. Some of these are notorious for antibiotic resistance, making treatment nightmarishly complex.
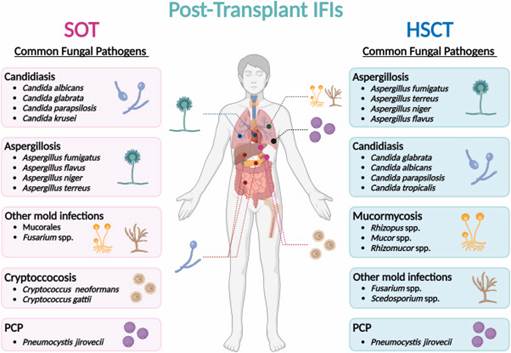
Fungal sepsis, though less frequent, carries an alarmingly high mortality rate. Candida species (Candida albicans, Candida glabrata) and Aspergillus fumigatus are among the primary fungal offenders, particularly in immunocompromised patients — those on chemotherapy, organ transplant recipients, or individuals with advanced HIV/AIDS.
Viral sepsis gained global attention with SARS–CoV-2 (COVID-19), but influenza, hantavirus, Ebola, and herpes simplex virus can all trigger a septic-like immune cascade. The COVID-19 pandemic gave the world an unwanted master class in what cytokine storms, a hallmark of sepsis, look like at epidemic scale.
The Terrible Complications: When Sepsis Attacks the Body
Sepsis doesn’t just cause fever and low blood pressure. It launches a systemic assault on virtually every organ system, producing complications that read like a medical horror story:
Disseminated Intravascular Coagulation (DIC) is among the most feared. The inflammatory cascade activates clotting pathways throughout the entire bloodstream simultaneously. Tiny clots, emboli, form in small blood vessels across organs, cutting off their oxygen supply. This can cause fingers, toes, and even limbs to die from ischemia, sometimes requiring amputation. Paradoxically, all these clotting factors get used up, and the patient then begins to bleed uncontrollably.
Septic emboli can seed heart valves, causing infective endocarditis, a condition in which bacteria or fungi colonize the delicate valve leaflets, forming destructive vegetations that can destroy valve architecture, cause the valve to leak or obstruct, and embolize clots to the brain, kidneys, and other organs.
Vascular complications include septic thrombosis in deep veins, mycotic aneurysms (weakening of arterial walls due to infection), and peripheral arterial occlusion. The systemic vasodilation that occurs in sepsis causes blood to pool inappropriately, crashing blood pressure and starving vital organs of perfusion.
Acute Respiratory Distress Syndrome (ARDS), acute kidney injury, liver failure, encephalopathy (brain dysfunction), and adrenal insufficiency round out the devastating catalog of sepsis complications.
Treating the Unknown Enemy: Empiric Therapy in Sepsis
Here is one of the most challenging aspects of sepsis management: when a patient arrives critically ill, you often don’t know what pathogen is causing it. Blood cultures take 24–72 hours to grow. Every hour of delay in starting antibiotics increases mortality by approximately 7–10%. So, physicians must act fast before the identity of the pathogen is confirmed.
This is called empiric antibiotictherapy, a calculated, educated bet based on the likely source of infection, the patient’s history, and local patterns of antibiotic resistance. The goal is broad-spectrum coverage: cast the net wide and catch the most likely offenders.
Common empiric antibiotic regimens include:
Piperacillin-tazobactam (Zosyn): a broad-spectrum penicillin-beta-lactamase inhibitor combination covering gram-negative rods, gram-positive organisms, and anaerobes.
Vancomycin: the gold standard for gram-positive coverage, particularly MRSA.
Meropenemor imipenem (carbapenems): “last-resort” broad-spectrum agents for highly resistant organisms or polymicrobial infections.
Cefepime or ceftriaxone: broad-spectrum cephalosporins for community-acquired or hospital-acquired infections.
Micafungin or fluconazole: added empirically when fungal sepsis is suspected, especially in immunocompromised patients.
Supportive care is equally critical: intravenous fluids to restore blood pressure, vasopressors (like norepinephrine) when fluids aren’t enough, supplemental oxygen and mechanical ventilation for respiratory failure, and dialysis for acute kidney injury. The “Surviving Sepsis Campaign” is an international initiative that has codified these interventions into evidence-based bundles of care, and adherence to these protocols measurably saves lives.
Despite all these tools, the fundamental problem remains: current treatments manage symptoms and fight the infection, but they do not address the underlying biological derangement — the molecular firestorm — that is actually killing the patient.
Enter Galectin-3: The Molecular Arsonist
Now we arrive at the biochemistry, the molecular heart of the story.
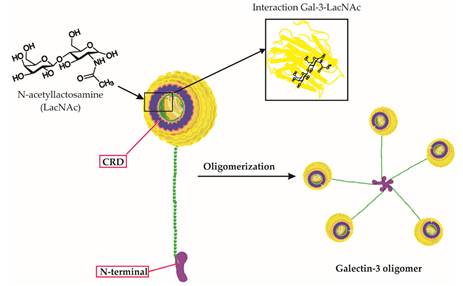
Galectin-3 (Gal-3) belongs to a family of proteins called lectins, which proteins that bind to specific sugar structures (carbohydrates) on the surfaces of cells and molecules. Think of lectins as the body’s molecular reading glasses: they scan the surface of cells, recognizing specific carbohydrate “words” and triggering biological responses accordingly.
Lectin Structure
Gal-3 was first identified and characterized in the 1980s. Researchers initially discovered it as a protein expressed on the surface of macrophages, the large immune cells that patrol the body eating cellular debris and pathogens. Early research identified it under several names: Mac-2 antigen, CBP35, L-29, and others, reflecting its discovery by multiple independent research groups before it was recognized as one and the same protein.
Structurally, Galectin-3 is unique among the galectin family. While most galectins have either one or two carbohydrate-recognition domains (CRDs), the sugar-binding “hands” of the protein, Galectin-3 has only one CRD, but it also possesses a long, flexible N-terminal domain. This tail allows multiple Galectin-3 molecules to self-assemble into oligomers, clusters of five or more molecules that form a lattice-like cage. This pentameric structure can crosslink multiple carbohydrate-bearing molecules simultaneously, effectively “stapling” cells, receptors, and signaling molecules together and amplifying inflammatory signals in a powerful, dangerous way.
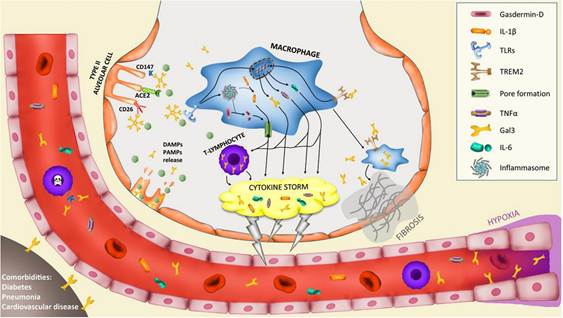
At the molecular level, Gal-3 binds to N-acetyllactosamine (LacNAc) disaccharide units, sugar structures found abundantly on the surface of immune cells, endothelial cells (cells lining blood vessels), and extracellular matrix components. When Gal-3 crosslinks these structures, it initiates intracellular signaling cascades involving NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells), a master regulator of inflammation. This triggers the release of pro-inflammatory cytokines including TNF-α, IL-1β, IL-6, and IL-8, the very molecules that drive the cytokine storm of sepsis.
In healthy physiology, Gal-3 plays constructive roles: it participates in wound healing, promotes phagocytosis (the eating of pathogens by immune cells), and helps regulate cell death. It is, in small amounts, a useful biological tool. But in serious infection, Gal-3 levels spike dramatically in the bloodstream. At high concentrations, it acts less like a tool and more like a match dropped in a gasoline-soaked room.
Specifically in sepsis, elevated circulating Gal-3 promotes uncontrolled macrophage activation, drives fibrosis in injured organs, amplifies neutrophil-mediated tissue damage, promotes the pro-coagulant state that leads to DIC and organ-destroying microemboli, and critically, impairs the body’s ability to resolve inflammation. It becomes, in essence, a molecular brake failure, preventing the immune system from switching off even after the infection is controlled.
Research has further established that Gal-3 is elevated in heart failure, acute kidney injury, liver fibrosis, and cancer, confirming its role as a central driver of inflammatory and fibrotic disease across multiple organ systems.
XGal-3: Engineering a Solution to a Molecular Problem
So if elevated Galectin-3 is a key driver of the sepsis catastrophe, what if you could simply remove it from the blood?
That is the elegantly straightforward premise of XGal-3®, a medical device developed by Eliaz Therapeutics, founded by Dr. Isaac Eliaz, a physician and researcher who has studied Galectin-3 for over three decades and whose own personal loss to immune dysregulation fueled a lifelong mission to combat it.
XGal-3® works on a principle similar to dialysis, but with a critical molecular twist. In standard dialysis, a patient’s blood is passed through a machine that filters out waste products using a semi-permeable membrane. XGal-3® uses therapeutic apheresis, a well-established clinical procedure, but instead of a generic membrane, the blood plasma passes through a column containing proprietary anti-Galectin-3 ligand traps: specially engineered molecules that selectively capture and remove Gal-3 from circulation. Think of it as a highly specific molecular fishing net, designed to catch only Galectin-3 while leaving everything else alone.
The device is designed to attach to existing apheresis machines, specifically the Terumo Spectra Optia® platform, already in widespread use in hospitals globally — making it potentially deployable without massive infrastructure investment.
What makes XGal-3® particularly remarkable from a scientific standpoint is that it removes both free and bound Gal-3 from circulation. In sepsis, Gal-3 exists in multiple forms in the bloodstream, free-floating molecules and molecules already crosslinked to cell-surface glycoproteins. The device’s engineered ligand traps capture both forms, offering a more comprehensive Gal-3 depletion than pharmacologic inhibitors, which typically only block the protein’s binding activity.
The early results are striking. In large animal studies, XGal-3® demonstrated the ability to halt the sepsis cascade within hours, a benchmark no currently approved treatment has achieved. Importantly, no adverse side effects were observed in these studies, a critical safety milestone. No serious complications have emerged in preclinical work, supported by two NIH grants totaling approximately $1.7 million and protected by over 60 patents across 34 countries.
The FDA has awarded XGal-3® its Breakthrough Device Designation, a status reserved for technologies that show promise for treating serious or life-threatening conditions where no adequate alternatives exist. This designation accelerates regulatory engagement and can shorten the path to market, giving critically ill patients potential access to this technology sooner.
Eliaz Therapeutics is now advancing toward investigator-led clinical trials in ICU settings at top academic medical centers, with the goal of demonstrating proof-of-concept in humans and building the evidence base needed for FDA approval.
The Bottom Line
Sepsis is a global killer that has eluded effective treatment because it has been approached primarily as an infection problem rather than an immune dysregulation problem. Galectin-3, a protein whose dangerous complexity is written into its very molecular architecture,appears to be one of the central conductors of the inflammatory orchestra that kills sepsis patients, even after the infection itself is controlled.
XGal-3® represents a conceptual leap: instead of drugging the immune system or fighting pathogens, it proposes removing a specific molecular instigator directly from the bloodstream. It is a marriage of extracorporeal medicine and precision molecular biology; dialysis meets targeted therapy.
Whether XGal-3® will fulfill its extraordinary promise will be answered in the clinical trials ahead. But what is already clear is this: the era of targeting the molecular roots of sepsis has arrived. And for the millions of patients who enter ICUs every year teetering on the edge of a storm they cannot see that may mean everything.
What pain management patients — and opioid-therapy advocates — need to know about buprenorphine’s hidden cost to oral health
Suboxone has become a contentious fixture of American medicine. Marketed primarily for opioid use disorder but increasingly pushed onto chronic pain patients, it carries a side effect that regulators were slow to acknowledge and many prescribers still downplay: rapid, severe dental decay. In 2022 the FDA added a warning to oral buprenorphine products after cataloging hundreds of cases of tooth loss, fractures, and cavities in patients with previously healthy mouths. This isn’t a hygiene failure; it’s chemistry, and it deserves a seat at the table alongside efficacy, withdrawal, and quality-of-life when weighing buprenorphine against a full-agonist opioid.
What Suboxone Actually Is
Suboxone combines buprenorphine with naloxone in a 4:1 ratio. Buprenorphine is the active agent; naloxone is an abuse deterrent that is poorly absorbed orally but blocks opioid receptors if the product is injected. Buprenorphine itself is available in several forms:
Sublingual films (Suboxone, Zubsolv) and tablets (Subutex, generic)
The dental risk is tied entirely to the oral formulations. The patch and injection bypass the oral cavity and show no comparable dental signal, which tells you the mechanism is local, not systemic.
Structure and Receptor Pharmacology
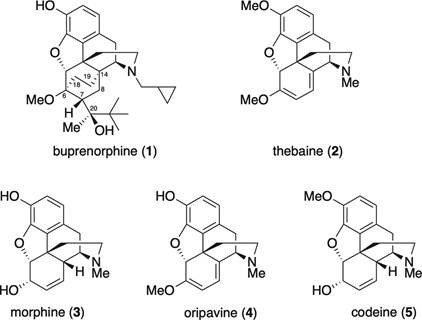
Buprenorphine is a semi-synthetic derivative of thebaine, an opium alkaloid. Structurally it retains the core morphinan scaffold shared by morphine, oxycodone, and hydrocodone — the rigid pentacyclic system with oxygen bridge, tertiary amine, and aromatic A-ring that defines classical mu agonists. Two modifications change everything: a bulky tert-butyl side chain at C7 and a cyclopropylmethyl group on the nitrogen. These increase lipophilicity dramatically and produce extraordinarily tight mu-receptor binding, with a dissociation half-life measured in hours.
Buprenorphine structure and comparisons
Buprenorphine docks into the same orthosteric pocket of the mu-opioid receptor that morphine does, contacting the same key residues (Asp147, Tyr148, His297). That homology is why it relieves pain and suppresses withdrawal.
The mu receptor is a class A G-protein coupled receptor. When a full agonist like morphine binds, two parallel intracellular events unfold. First, the Gαi/o subunit dissociates and inhibits adenylyl cyclase, dropping cyclic AMP, while Gβγ opens GIRK potassium channels and closes voltage-gated calcium channels, hyperpolarizing neurons and blunting neurotransmitter release. That is the analgesic arm. Second, the receptor is phosphorylated by GRK kinases and recruits beta-arrestin-2, which drives internalization, desensitization, and much of the respiratory depression, constipation, and tolerance attributed to opioids.
Buprenorphine is a partial agonist at mu: higher affinity than morphine but only partial G-protein activation, producing the ceiling effect on respiratory depression. It is also a biased ligand, recruiting beta-arrestin-2 poorly, and it antagonizes the kappa receptor while partially engaging the nociceptin receptor. Pharmacologically elegant. Dentally, irrelevant.
The Dental Damage: A Chemical, Not Behavioral, Problem
Tooth enamel is hydroxyapatite — Ca₁₀(PO₄)₆(OH)₂ — a crystalline mineral that dissolves whenever the pH at its surface drops below 5.5. The mouth is normally buffered near neutral by saliva, which is supersaturated with calcium and phosphate and rich in bicarbonate. Every acid challenge from food or drink is neutralized within minutes, and minerals are redeposited. This remineralization is what keeps teeth intact across a lifetime.
Suboxone disables the system in four simultaneous ways.
1. The drug itself is acidic
Buprenorphine films and tablets are formulated at low pH for solubility and stability. Dissolved in saliva, they drop the local pH to 3.5–4.5, which is well below the critical threshold. Hydrogen ions penetrate the hydroxyapatite lattice, protonate phosphate groups, and liberate calcium into saliva. This is straight acid etching, the same chemistry used to dissolve limestone.
2. Contact time is prolonged
A film takes 10 to 30 minutes to dissolve, and patients are told not to rinse or swallow excessively during absorption. The acid bath sits against enamel far longer than anything else people put in their mouths.
3. Saliva production crashes
Mu-opioid receptors in the brainstem salivary nuclei and on parasympathetic fibers to the salivary glands suppress acetylcholine release when activated, cutting salivary flow by 50 to 75 percent in chronic users. No saliva means no bicarbonate buffer, no calcium-phosphate reservoir, and no mechanical clearance. The remineralization arm of the equation is amputated.
4. The microbiome shifts and the pellicle thins
Dry, acidic mouths favor aciduric bacteria like Lactobacillus, which ferment residual carbohydrate through glycolysis to lactic acid (pKa 3.86). Meanwhile, amphipathic buprenorphine molecules adsorb onto enamel and displace the salivary proteins (statherin, mucins, proline-rich proteins) that form the protective acquired pellicle. The barrier thins, and protons penetrate more easily.
The cumulative effect is catastrophic. Reports describe patients losing multiple teeth within one to two years of starting Suboxone, with decay at unusual sites — cervical margins, incisal edges, between teeth — rather than the usual occlusal pits. These patterns are pathognomonic for chemical erosion, not ordinary bacterial caries.
How Suboxone Compares to Other Opioids
Advocates for traditional opioid therapy often ask whether their preferred medications cause the same damage. The answer is largely no — and the reasons are instructive.
Factor
Suboxone (sublingual)
Oral full-agonist opioids
Oral contact time
10–30 minutes of dissolution
Seconds; swallowed whole
Local pH at tooth surface
3.5–4.5
Near neutral
Dry mouth effect
Strong, chronic
Present but typically milder
FDA dental warning
Yes (2022)
No equivalent class warning
Oral morphine, oxycodone, and hydrocodone all cause some xerostomia through the same central mechanism, and long-term opioid users do show elevated caries rates. But without the direct acid bath and prolonged mucosal contact, damage is slower, more diffuse, and more responsive to ordinary hygiene. Methadone liquid — often sweetened and sipped slowly — produces a pattern closer to Suboxone. Transdermal buprenorphine and the Sublocade injection avoid the oral hit entirely and show no comparable dental signal.
Prevention: What Actually Works
If you are on sublingual buprenorphine and intend to stay on it, the biochemistry dictates the countermeasures: shorten acid exposure and restart remineralization as quickly as possible after each dose.
Do not rinse, brush, or drink immediately before dosing. You need saliva present to dissolve the drug.
After the film or tablet is fully dissolved, wait a few minutes, then rinse with plain water or a diluted baking soda solution (½ teaspoon in a cup of water). Bicarbonate neutralizes residual acid and raises pH above the critical threshold.
Do not brush for at least 30 minutes afterward. Softened enamel is physically removed by abrasive brushing at that moment.
Use a prescription 5,000 ppm fluoride toothpaste at bedtime. Fluoride substitutes into the lattice as fluorapatite, which resists dissolution to pH 4.5.
Add a calcium-phosphate remineralizing agent (CPP-ACP, sold as MI Paste). It replaces the ions the drug strips out.
Treat dry mouth aggressively. Xylitol gum stimulates saliva and inhibits S. mutans; pilocarpine or cevimeline can be prescribed for severe cases.
See a dentist every three to four months, not every six. Early white-spot lesions are reversible; cavitated lesions are not.
Discuss non-oral formulations with your prescriber. The Sublocade injection and Butrans patch deliver buprenorphine without touching enamel.
The Bottom Line
The case against Suboxone’s dental profile isn’t a talking point. It is chemistry you can measure with pH paper. A partial mu agonist with fascinating receptor-level biology has been delivered in a vehicle that bathes teeth in acid for half an hour at a time while simultaneously switching off the body’s repair system. That design choice was made for pharmacokinetic convenience, not patient welfare, and the consequences are visible in thousands of mouths.
For pain patients considering their options, and for advocates arguing the pendulum has swung too far toward buprenorphine and away from traditional opioid therapy, this is a legitimate piece of the argument. Informed consent means knowing that the price of the ceiling effect on respiratory depression may, for some people, be their teeth, and that cheap countermeasures exist if you start using them from day one. Talk to your dentist before your next refill.
What does the research actually say about these trending compounds — and are they worth adding to your stack?
Few categories in the wellness world straddle the ancient and the cutting-edge quite like adaptogens. Rooted in thousands of years of Ayurvedic and Traditional Chinese Medicine, these botanical compounds have recently attracted serious attention from researchers, longevity clinicians, and biohackers looking for evidence-based tools to manage chronic stress, sharpen cognition, and optimize hormonal health. But the question worth asking with the rigor the topic deserves is: does the science hold up?
What Exactly Is an Adaptogen?
The term “adaptogen” was coined by Soviet pharmacologist Nikolai Lazarev in 1947 and later refined by his colleague Israel Brekhman. To qualify as an adaptogen, a substance must meet three criteria: it must be non-toxic at normal doses; it must produce a nonspecific resistance to stress, meaning it helps the body cope with a broad range of physical, chemical, and biological stressors; and it must help restore physiological balance, or homeostasis, regardless of the direction of the deviation.
Example of Adaptogens
This last criterion is particularly fascinating from a pharmacological standpoint. Unlike most drugs, which push a biological variable in one direction, adaptogens are described as “bidirectional” in that they tend to normalize function. An adaptogen that influences cortisol, for example, may lower it when chronically elevated and support it when depleted. This homeostatic quality is mechanistically distinct from stimulants, sedatives, or simple hormone precursors.
The Mechanism: How Adaptogens Work at the Cellular Level
Modern research has begun to illuminate the molecular pathways behind these effects, and the biochemistry is genuinely interesting. Adaptogens appear to work primarily through three interrelated systems:
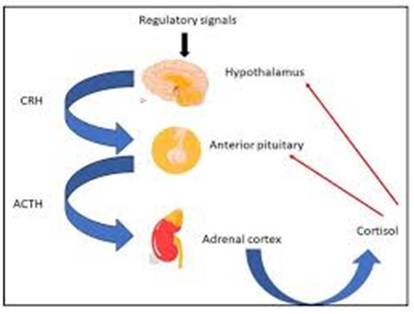
1. The HPA Axis (Hypothalamic-Pituitary-Adrenal)
The HPA axis is the body’s central stress-response network. When a stressor is perceived, the hypothalamus releases corticotropin-releasing hormone (CRH), which signals the pituitary to release adrenocorticotropic hormone (ACTH), which in turn drives the adrenal cortex to secrete cortisol. This cascade is adaptive in short bursts, but chronic activation leads to dysregulation, inflammation, metabolic disruption, and immunosuppression. Several adaptogens, particularly Ashwagandha (Withania somnifera) and Rhodiola rosea, have been shown to modulate this axis, reducing the cortisol output under conditions of chronic psychological stress.
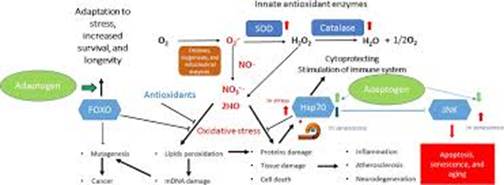
2. The SAS (Sympatho-Adrenal System) and Molecular Chaperones
A landmark paper by Panossian and Wikman (2010) proposed that adaptogens act on stress sensor proteins, particularly Hsp70 (heat shock protein 70) and nitric oxide (NO), which serve as molecular “early warning systems” that detect cellular stress before it becomes systemic. Adaptogens appear to trigger a mild, hormetic stress response that upregulates protective proteins like Hsp70 and Hsp90, essentially pre-conditioning the cell to handle more significant stressors. This hormesis model, small stress, big resilience, echoes the principle behind cold exposure and high-intensity interval training.
3. Neuroprotection and Cognitive Pathways
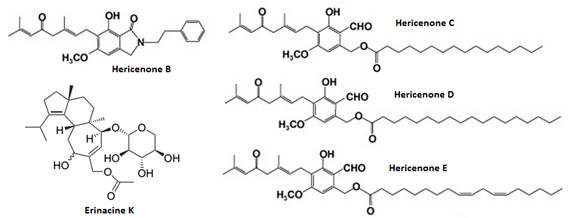
Several adaptogens interact with neurotransmitter systems involved in mood, attention, and neuroprotection. Bacopa monnieri appears to enhance synaptic communication by modulating serotonin and acetylcholine pathways and may support neurogenesis via BDNF (brain-derived neurotrophic factor) upregulation. Lion’s Mane mushroom (Hericium erinaceus) has attracted significant attention for its ability to stimulate Nerve Growth Factor (NGF) synthesis, a key signaling protein in neuron maintenance and plasticity through bioactive compounds called hericenones and erinacines.
Lions Mane
Compounds in Lions mane (hericenones and erinacines) which stimulate the production of Nerve Growth Factor.
Cortisol Management: The Data
Cortisol dysregulation is implicated in anxiety, poor sleep, abdominal fat accumulation, immune suppression, and accelerated biological aging, so it is no surprise this is where adaptogen research has concentrated. The most compelling human clinical data currently belongs to Ashwagandha. A double-blind, randomised controlled trial published in Medicine (2019) found that 240 mg/day of a standardised Ashwagandha extract produced a statistically significant 23% reduction in serum cortisol levels compared to placebo over 60 days, alongside improvements in self-reported stress scores, sleep quality, and memory performance.
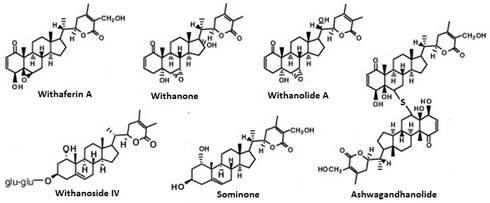
Ashwagandha
The active constituents in Ashwagandha, withanolides, a class of steroidal lactones, are thought to inhibit the NF-κB inflammatory pathway and modulate GABA receptor activity, which may explain both the anxiolytic and cortisol-modulating effects. This is not merely folk medicine; it is identifiable receptor-level pharmacology.
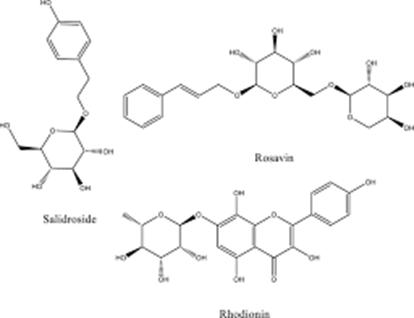
Rhodiola rosea, rich in rosavins and salidroside, has similarly demonstrated cortisol-modulating properties, particularly in the context of burnout and fatigue. A 2022 systematic review in Phytomedicine examining 36 studies found consistent evidence for Rhodiola’s ability to reduce perceived fatigue and improve mental performance under stress — though the authors noted that study quality and standardisation vary considerably across the literature.
Rhodiola Rosea
Rosavins and Salidroside Chemical Structures
You can find and purchase Rhodiola Rosea supplement here on Amazon –> https://amzn.to/4sXDo4h
Mental Clarity, Cognition, and Neuroprotection
Beyond stress hormones, the cognitive applications of adaptogens are a growing area of legitimate inquiry. Bacopa monnieri has arguably the most robust human trial data for cognitive enhancement of any herbal compound — multiple randomised controlled trials have demonstrated improvements in spatial working memory, information processing speed, and delayed word recall, typically with chronic supplementation over 8–12 weeks. The mechanism involves antioxidant effects in the hippocampus, acetylcholinesterase inhibition, and modulation of dopaminergic neurotransmission.
Lion’s Mane mushroom is particularly interesting to the longevity community because its NGF-stimulating properties position it as a potential neuroprotective agent. Preclinical evidence is strong. Human trials are fewer, but a 2009 double-blind RCT in Phytotherapy Research found that 1,000 mg/day of Lion’s Mane over 16 weeks produced significant improvements in cognitive function scores in older adults with mild cognitive impairment, with effects reversing upon cessation — suggesting a dependency on continued supplementation rather than permanent neurological modification.
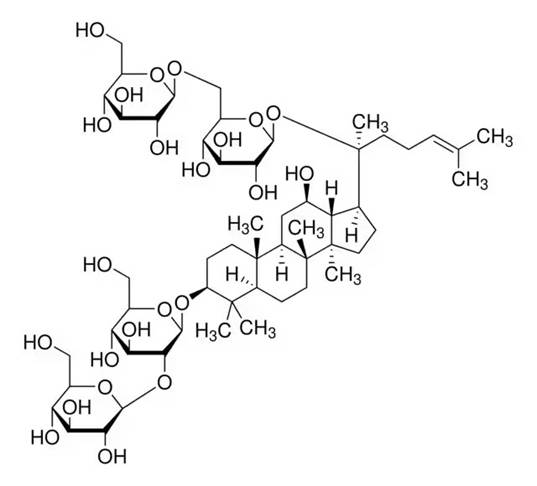
The adaptogen category is broader than stress and cognition alone. Panax ginseng (Asian ginseng) has accumulated substantial evidence for immune modulation, exercise performance enhancement, and glycemic support; ginsenosides appear to sensitise insulin receptors and support mitochondrial ATP production. Eleuthero (Siberian ginseng), while technically not a true ginseng, has been studied for its effects on endurance and immune resilience, particularly in Soviet-era athletic research (though much of this data requires modern replication).
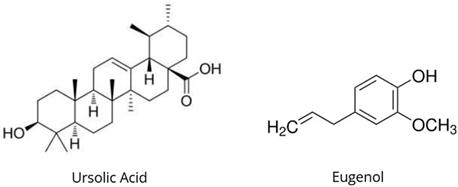
Schisandra chinensis, used extensively in Traditional Chinese Medicine, has shown hepatoprotective properties via upregulation of glutathione synthesis, and has been studied for its potential in supporting liver enzyme normalisation in individuals with non-alcoholic fatty liver disease. Holy Basil (Ocimum tenuiflorum), or Tulsi, is being explored for its anti-inflammatory and thyroid-supporting properties, with compounds like eugenol and ursolic acid inhibiting COX-2 enzyme activity — the same target as ibuprofen.
This is the question that separates informed supplementation from wishful thinking. The honest answer is: it depends on the compound. The evidence base is uneven. Ashwagandha and Bacopa have multiple high-quality RCTs with good blinding and standardized extracts. Rhodiola has decent mechanistic and human data. Lion’s Mane is promising but still thin on large-scale human trials. Many lesser-known adaptogens have weak or absent human data despite compelling in vitro or animal findings.
Key limitations to be aware of: dosing and extract standardization are highly variable between studies, making meta-analyses difficult. Funding bias exists, with some trials sponsored by supplement manufacturers. Effect sizes, while often statistically significant, are frequently modest in absolute terms — meaningful for chronic management, less so for acute performance. And placebo response in stress and cognition studies is substantial, making trial design particularly demanding.
That said, dismissing adaptogens as purely anecdotal misreads the current state of the literature. For the top-tier compounds, there is now mechanistic plausibility at the receptor and signaling pathway level, corroborated by human clinical data of sufficient quality to inform clinical recommendations — a bar that many pharmaceutical interventions for stress and cognition have not cleared either.
Practical Considerations for Biohackers
If you are considering adding adaptogens to your protocol, a few principles are worth noting. First, these are chronic, not acute, interventions —the strongest effects emerge after weeks of consistent use, not hours. Second, sourcing matters enormously; look for standardised extracts (e.g., KSM-66 for Ashwagandha (Buy here-à https://amzn.to/4bhXUXk , Bacognize for Bacopa) with verified withanolide or bacosides content, third-party tested. Third, adaptogen effects may be subtle and cumulative rather than dramatic, making them well-suited to longevity-oriented stacks rather than acute performance enhancement.
Finally, the bidirectional, homeostatic nature of these compounds means context matters. If your cortisol is normal, the cortisol-lowering effects of Ashwagandha will be attenuated. The most profound benefits appear in individuals with measurable dysregulation — chronic stress, impaired sleep architecture, or declining cognitive performance — which is consistent with the homeostatic mechanism proposed in the literature.
The Bottom Line
Adaptogens occupy a genuinely interesting and scientifically credible space in the wellness landscape. They are not panaceas, and the field is not without its flaws, but the mechanistic picture emerging from molecular biology and the clinical signals from better-designed trials suggest that the right compounds, in the right doses, from quality sources, can provide meaningful support for stress resilience, cortisol regulation, and cognitive longevity. In a world of chronic stressors and overstimulated nervous systems, that is not nothing — it might, in fact, be exactly the kind of low-risk, high-signal tool a well-designed longevity protocol has been missing.
Key Compounds at a Glance
Ashwagandha (Withania somnifera): Cortisol reduction, anxiety, sleep quality, thyroid support
Rhodiola rosea: Fatigue reduction, burnout, mental performance under stress
Holy Basil (Tulsi): Anti-inflammatory (COX-2), stress adaptation, immune function
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning any supplementation protocol.
A Plain-English Guide to Understanding Scientific Research
You’ve seen the headlines: “Study Links Coffee to Longer Life” or “New Research Suggests Red Wine Prevents Heart Disease.” A week later, a contradictory headline appears. How can science keep flip-flopping? The answer, more often than not, isn’t that the science is broken; it’s that not all studies are built the same. Understanding the different types of scientific research is one of the most useful thinking tools you can develop. Let’s break it down.
The Gold Standard: The Randomized Controlled Trial (RCT)
If scientific studies were currencies, the randomized controlled trial (RCT) would be gold bullion. Here’s how it works: researchers take a group of participants and randomly assign them to either receive a treatment (the experimental group) or not (the control group). Random assignment is the magic ingredient; it helps ensure the two groups are as similar as possible, so any difference in outcomes can be attributed to the treatment itself.
What it’s great at: Establishing causation — not just that two things are correlated, but that one actually causes the other. If a new drug reduces blood pressure in an RCT, you can be fairly confident the drug is doing the work.
What it’s not great at: RCTs are expensive, time-consuming, and sometimes ethically impossible. You can’t randomly assign people to smoke cigarettes for 20 years to study lung cancer. They’re also often conducted on narrow populations that may not represent everyone.
Blinding the Study: Single, Double, and Triple-Blind Trials
Even in a well-designed RCT, human psychology can sneak in and distort results. That’s where blinding comes in.
In a single-blind study, participants don’t know which group they’re in — they don’t know if they’re getting the real treatment or a placebo. This helps prevent the placebo effect, where simply believing you’re receiving treatment can make you feel better.
In a double-blind study, neither the participants nor the researchers know who is in which group. This is considered the most rigorous standard for clinical trials. Some studies go even further with triple-blinding, where even the statisticians analyzing the data don’t know which group is which until the analysis is complete.
What it’s great at: Minimizing bias from both participants and researchers — some of the most insidious sources of error in science.
What it’s not great at: Blinding isn’t always possible. You can’t blind someone to whether they received surgery or not, or whether they changed their diet. Even double-blind trials can be “unblinded” if a drug has obvious side effects that reveal who’s in the treatment group.
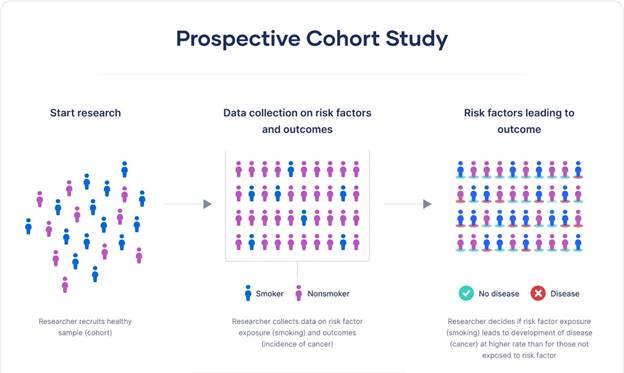
Prospective Studies: Following People Forward in Time
A prospective study starts before the outcome of interest has occurred and follows participants forward in time to see what happens. Researchers identify a group (called a cohort), collect baseline information, and then track them over months or years.
The famous Nurses’ Health Study, launched in 1976, is a classic example. Researchers enrolled over 120,000 nurses and tracked their health behaviors and outcomes for decades. This kind of long-term follow-up has produced enormous insights into diet, lifestyle, and disease.
What it’s great at: Studying how exposures like diet or exercise relate to health outcomes. Because data is collected as events unfold, recall bias — the tendency to misremember past events — is reduced.
What it’s not great at: They’re expensive and slow. If you want to study a disease that takes 20 years to develop, you might wait 20 years for answers. They also can’t prove causation the way RCTs can, because participants aren’t randomly assigned to their exposures.
Retrospective Studies: Looking Backward
A retrospective study does the opposite — it starts with an outcome that has already occurred and looks backward to identify possible causes or risk factors. Researchers might study a group of people who already have a disease and compare their past exposures to a group without the disease.
What it’s great at: Speed and cost. Since you’re working with existing data or records, you can complete a study in months rather than decades. Particularly useful for rare diseases, where waiting for prospective cases would take too long.
What it’s not great at: Prone to recall bias — people remember their past differently depending on their current health. A person who developed cancer may scrutinize their past habits very differently than a healthy person.
Case -Control Studies: Comparing Cases to Controls
A case-control study is a type of retrospective study that specifically compares people with a condition (cases) to people without it (controls), looking backward to compare their exposures. It’s particularly useful for rare diseases — rather than enrolling tens of thousands and waiting, you find 100 people who already have the condition, match them to 100 similar people who don’t, and compare their histories.
What it’s great at: Efficiency when studying rare conditions or diseases with long latency periods.
What it’s not great at: Selecting the right control group is tricky and can introduce bias. They also share the retrospective study’s weakness of recall bias.
Cross-Sectional Studies: A Snapshot in Time
A cross-sectional study is like a photograph — it captures data from a population at a single point in time. National health surveys, for example, might ask thousands of people about their diet, exercise, and health status simultaneously.
What it’s great at: Efficiently describing the prevalence of conditions or behaviors across a population. Excellent for public health planning.
What it’s not great at: Because everything is measured at one moment, you can’t determine whether the exposure came before or after the outcome. Does depression cause physical inactivity, or does physical inactivity cause depression? A cross-sectional study can’t tell you.
Observational vs. Experimental Studies: The Big Divide
It’s worth stepping back to note the most fundamental distinction in research: observational versus experimental studies.
In observational studies (like prospective, retrospective, and cross-sectional studies), researchers observe people as they live their lives without intervening. They can find associations and correlations, but proving causation is always more difficult.
In experimental studies (like RCTs), researchers actually do something — they assign treatments, change variables, and measure what happens. This is why RCTs are so valued: intervention + randomization = the best shot at establishing cause and effect.
Meta-Analyses and Systematic Reviews: The View from 30,000 Feet
What happens when you have dozens of individual studies on the same question and they don’t all agree? Enter the systematic review and its statistical cousin, the meta-analysis.
A systematic review is a rigorous, exhaustive summary of all the available research on a specific question. Researchers search databases methodically, apply strict inclusion criteria, and synthesize what the evidence shows as a whole.
A meta-analysis goes one step further: it statistically combines the data from multiple studies to produce a single, pooled estimate. This dramatically increases the effective sample size and statistical power.
What they’re great at: Giving you the big picture. A single study might show a drug works; a meta-analysis of twenty studies gives you much greater confidence — or might reveal that the positive results were an anomaly.
What they’re not great at: “Garbage in, garbage out.” If the underlying studies are flawed, combining them doesn’t fix those flaws — it might just obscure them. Meta-analyses can also be manipulated by cherry-picking which studies to include.
Peer Review: The Gatekeeper (With Flaws)
You’ve probably heard the term peer-reviewed study used as a badge of credibility. Peer review means that before a study is published in a scientific journal, it is evaluated by independent experts in the same field who assess its methodology, analysis, and conclusions. It’s a critical quality-control mechanism.
What it’s great at: Catching obvious errors, methodological problems, and unsupported conclusions before they reach the public.
What it’s not great at: Peer review is not infallible. Reviewers are human, biased, and usually unpaid volunteers working with limited time. High-profile journals have published studies that were later retracted. Peer review filters out the worst work, but it doesn’t guarantee truth.
Putting It All Together
The next time you read about a new study, ask a few key questions: Was it observational or experimental? How many people were involved? Was it peer-reviewed? Has it been replicated? A single observational study showing a correlation between two things is interesting — but it’s just a starting point. Confidence builds when multiple types of studies, done by different research teams, in different populations, point in the same direction.
Science isn’t a collection of facts — it’s a process of accumulating evidence. Knowing how that process works makes you a far better reader of it.
By the time principal dancer Misty Copeland announced her retirement and shared a candid video of her post-surgical recovery — appearing to show rehabilitation following hip surgery — the ballet world had witnessed what many already understood: that a career at the pinnacle of classical dance exacts a profound physical cost. Copeland, who made history as the first African American female principal dancer at American Ballet Theatre, danced through injuries that would have ended most careers. Her public recovery pulled back the curtain on a reality that elite ballerinas know intimately but rarely discuss: the human body was not designed for the demands of professional ballet, and it pays dearly for decades of attempting the impossible.
While audiences marvel at the effortless grace of a ballerina suspended en pointe, orthopedic surgeons see something else: a skeleton stressed beyond its anatomical limits, joints compressed at angles evolution never intended, and connective tissue in a perpetual state of micro-trauma. The foot and ankle injuries associated with pointe work are well known, but they represent only part of the story. From the lumbar spine to the hip socket, from the knee to the sacroiliac joint, ballet extracts damage at every level of the musculoskeletal system.
The Hip: Ballet’s Most Demanding Joint
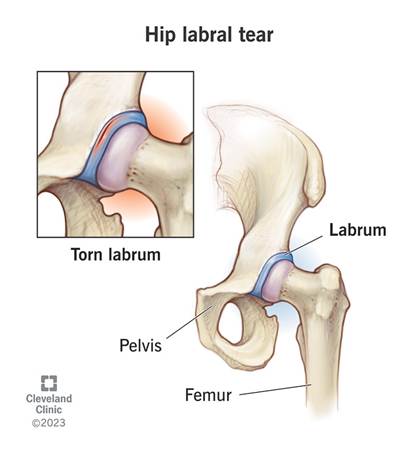
The hip is ground zero for the kind of catastrophic wear that Copeland’s recovery video seemingly illustrates. Ballet’s foundational aesthetic principle — turnout, the external rotation of both legs from the hip socket — places extraordinary demands on the acetabular labrum, the ring of cartilage that deepens the hip socket and stabilizes the femoral head. Elite dancers spend years forcing their hips into ranges of rotation that exceed what the joint anatomy typically allows, and the labrum bears the brunt of this.
Labral tears are endemic among professional ballet dancers. Studies suggest rates as high as 80 to 90 percent among elite dancers who undergo hip imaging, though many tears remain asymptomatic until the cumulative damage reaches a tipping point. When symptoms emerge — deep groin pain, a clicking or catching sensation, pain with hip flexion or external rotation — they signal structural compromise that often requires surgical intervention, typically arthroscopic labral repair or reconstruction.
Beyond labral pathology, elite dancers are susceptible to femoroacetabular impingement (FAI), a condition in which bony prominences on the femoral head or acetabular rim create abnormal contact during movement. The forced extremes of ballet — deep plié, grand battement, arabesque — grind these surfaces together repeatedly, producing progressive cartilage erosion that can lead to early-onset osteoarthritis of the hip. Some former dancers undergo total hip replacement in their forties, decades earlier The Knee: Bearing the Load of Every Landing
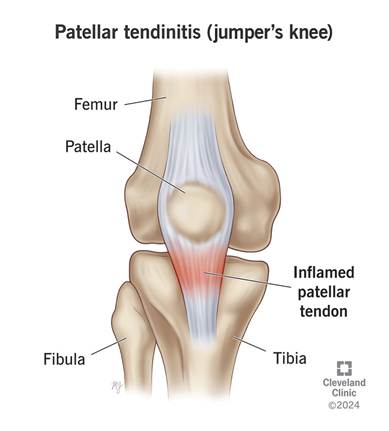
Every jump in ballet ends with a landing and the knee absorbs the shock. In professional ballet, a dancer may execute hundreds of jumps per rehearsal day, each one concentrating forces of three to five times body weight through the knee joint. Over a career spanning fifteen to twenty years at the professional level, this cumulative loading creates predictable patterns of injury and degeneration.
Patellar tendinopathy, colloquially known as jumper’s knee, is one of the most common overuse injuries in ballet. The repeated eccentric loading of the quadriceps during landing produces microtrauma within the patellar tendon that, if insufficiently recovered, progresses to chronic tendon degeneration. Anterior knee pain from patellofemoral syndrome is equally prevalent, arising partly from the external rotation demands of turnout, which alter the tracking mechanics of the patella and increase lateral compartment pressure.
Meniscal damage follows a similar pattern to hip labral tears: gradual wear that accumulates invisibly until a threshold is crossed. The medial and lateral menisci, which act as shock absorbers and stabilizers within the knee, are subject to compressive and shear forces during the deep plié positions ballet demands. Partial meniscal tears, once managed conservatively, may ultimately require surgical intervention and frequently herald early-onset knee osteoarthritis.
The Spine: Dancing Through Compression and Instability
The demands placed on a ballerina’s spine are contradictory and unforgiving. Ballet simultaneously requires extreme lumbar extension, the arched back of an arabesque and the postural discipline of a perfectly vertical torso in fifth position. This oscillation between hyperlordosis and strict alignment, repeated across thousands of hours of training, creates a unique spinal stress profile.
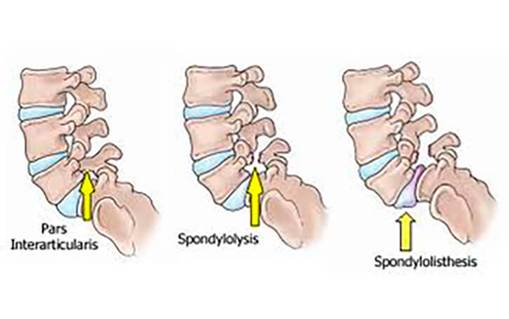
Spondylolysis, a stress fracture of the pars interarticularis, a small bridge of bone between vertebral facet joints, occurs at significantly elevated rates among ballet dancers compared to the general population. The repetitive hyperextension of arabesque and attitude positions creates cyclical stress at the posterior elements of the lumbar spine, particularly at L4 and L5. Bilateral spondylolysis can progress to spondylolisthesis, in which a vertebra slips forward relative to the one below it, causing chronic back pain and nerve root compromise.
Intervertebral disc pathology is also common, driven both by the compressive loads of partnering, where male dancers lift ballerinas repeatedly overhead, and by the chronic postural demands of training. Herniated discs, most frequently at L4-L5 and L5-S1, can produce radiculopathy that radiates down the leg, threatening not just a dancer’s comfort but her technical capability and career longevity.
The Foot and Ankle: Where Dance Meets Damage
No discussion of ballet injuries is complete without the foot, and though this territory is well mapped, its severity bears emphasis. Dancing en pointe, the practice of supporting the full body weight on the tips of the toes, is perhaps the most anatomically radical thing a human being can routinely do. The metatarsophalangeal joints, the sesamoid bones beneath the first metatarsal, and the entire bony architecture of the forefoot are subjected to loading conditions that have no parallel in normal human movement.
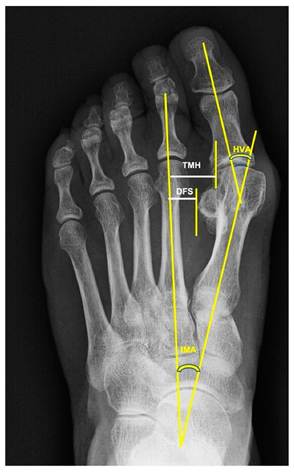
Hallux valgus — the lateral deviation of the great toe, is nearly universal among female ballet dancers who have danced on pointe for many years. The pointe shoe itself compresses the forefoot, and the mechanical demands of pointe work drive progressive angular deformity at the first metatarsophalangeal joint. Bunion formation, joint capsule thickening, and progressive articular cartilage loss in this joint create painful limitations that worsen after retirement when the protective conditioning of active training is lost.
Hallux Valgus
Posterior impingement syndrome, caused by compression of soft tissue or an accessory os trigonum bone between the back of the tibia and the calcaneus during full plantarflexion, is another characteristically ballet-specific condition. Ankle instability from recurrent sprains, Achilles tendinopathy from the relentless demand placed on the calf complex, and stress fractures of the metatarsals and navicular round out a formidable inventory of foot pathology.
The Systemic Dimension: When Bone Density Becomes the Enemy
Underpinning many of these musculoskeletal injuries is a systemic vulnerability that the dance world has been slow to confront: the Female Athlete Triad. The combination of low energy availability driven by the aesthetic pressure to maintain extreme leanness, menstrual dysfunction, and diminished bone density creates a physiological environment in which bones are structurally compromised even as they are placed under extraordinary mechanical demand. Stress fractures, which might be merely inconvenient in an athlete with adequate bone density, become potentially career-ending events in dancers whose bones are prematurely osteopenic.
Research published in journals including the British Journal of Sports Medicine has documented lower bone mineral density in ballet dancers compared to age-matched controls, despite the weight-bearing nature of their activity, which would ordinarily be protective. The culprit is hormonal disruption from chronic energy restriction, which suppresses estrogen and impairs the osteoblastic activity needed to maintain bone density. The result is a dancer whose skeleton, despite extraordinary muscular development and technical mastery, is more fragile than it should be.
The Cultural Reckoning
What makes these injuries particularly poignant is their inevitability within the current structure of professional ballet. The training begins in childhood, typically between ages eight and twelve, when skeletal development is still incomplete and growth plates remain vulnerable. The aesthetic standards of the classical repertoire have changed little in a century. The pressure to perform through pain is embedded in the culture of most major companies, where taking a rest day can mean losing a role to a competitor waiting in the wings.
Misty Copeland’s willingness to document her surgical recovery publicly represents something genuinely new in this culture: the acknowledgment, by one of ballet’s most celebrated figures, that the body eventually presents its bill. Her recovery video is not an admission of weakness but an act of transparency — and perhaps an invitation for the art form to reckon honestly with what it costs its practitioners.
The grace that fills the stage at Lincoln Center or the Paris Opéra is real, but it is purchased at a price measured in labral tears and herniated discs, in bunioned feet and vertebral stress fractures, in joints worn decades beyond their years. Understanding that price is the first step toward demanding something better — better medical support, more honest conversations about physical limits, and an aesthetic evolution that might allow extraordinary artists to give more of their lives to their art.
A Quiet Discovery Out of Germany Could Change Everything We Know About Osteoporosis
For decades, the conversation around osteoporosis treatment has felt a bit like a losing battle. You take calcium. You get enough vitamin D. You lift weights. You hope for the best. Current medications can slow bone loss, but many come with serious long-term side effects and none of them truly rebuild bone from the inside out the way your body naturally would in its prime.
That may be about to change.
Researchers at Leipzig University in Germany have identified a little-known molecular “switch” on bone cells, a receptor called GPR133 that, when activated, can dramatically boost bone formation, reverse osteoporosis-like bone loss, and even amplify the benefits of exercise. The compound they used to flip that switch? A molecule called AP503. And the results in mice have been striking enough to turn heads across the scientific community.
Who Made This Discovery — and Where?
The work was led by Professor Ines Liebscher, MD, PhD, a researcher at the Rudolf Schönheimer Institute of Biochemistry within Leipzig University’s Faculty of Medicine. Her lab has spent more than a decade focused on a still-underexplored family of proteins called adhesion G protein-coupled receptors (aGPCRs), a class of cell-surface receptors that act like biological antennas, translating physical forces and chemical signals from the outside world into instructions the cell can act on.
The lead author of the most recent bone study is Dr. Juliane Lehmann, also based at Leipzig’s Biochemistry Institute. Their work is embedded within Collaborative Research Centre 1423, a major scientific initiative dedicated to understanding the structural dynamics of GPCR activation and signaling. Leipzig is internationally recognized as one of the leading centers for this specialized area of molecular biology.
Importantly, the research has international reach. An earlier study by the Liebscher group conducted in collaboration with Shandong University in China had already shown that activating GPR133 with AP503 strengthens skeletal muscle. The new bone findings build naturally on that earlier discovery, painting an increasingly compelling picture of GPR133 as a master regulator of musculoskeletal health.
What Exactly Is GPR133, and Why Does It Matter?
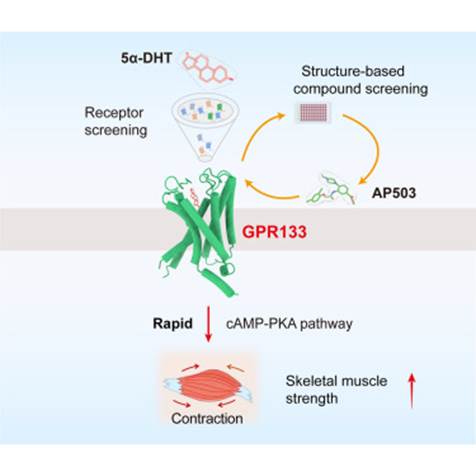
GPR133 (also known as ADGRD1) is a receptor that sits on the surface of bone-forming cells called osteoblasts. Think of it as a sensory hub: it detects two distinct signals simultaneously, physical mechanical strain (the kind that comes from movement and exercise) and a molecular partner called PTK7, which is presented by neighboring cells.
When both signals arrive together, GPR133 fires. It triggers a cascade inside the cell: levels of cyclic AMP (cAMP) rise, which activates enzymes that ultimately switch on the β-catenin signaling pathway, a well-known driver of bone-building gene programs. The result is more osteoblast activity, more new bone formation, and, critically, less osteoclast activity (osteoclasts are the cells that break bone down). Bones become denser and stronger.
When the researchers genetically removed GPR133 from mice entirely, those animals developed thin, weak bones early in life, eerily similar to human osteoporosis. That finding alone validated GPR133 as a meaningful player in bone health. Human genome-wide association studies had previously linked GPR133 gene variants to differences in bone mineral density and even body height, but this was the first deep mechanistic look at exactly how and why.
Enter AP503: A Compound That Mimics the Body’s Own Signal
AP503 was identified through a computer-assisted screening process, essentially a sophisticated computational search designed to find small molecules capable of activating GPR133. It is classified as a selective receptor agonist, meaning it binds to GPR133 and mimics the natural activation that normally requires both mechanical force and PTK7 signaling.
When healthy mice received daily injections of AP503, their bone volume and strength increased measurably. When mice engineered to model postmenopausal osteoporosis (via ovariectomy, which removes estrogen) received the compound, the bone loss was significantly reversed, osteoblast counts improved and signs of bone resorption eased. Critically, when AP503 was combined with treadmill exercise, the effects were synergistic: the two together outperformed either intervention alone. That biological partnership between movement and a targeted molecule is exactly the kind of finding that excites longevity researchers.
As Dr. Lehmann noted, the newly demonstrated parallel strengthening of bone — building on their earlier muscle research — “highlights the great potential this receptor holds for medical applications in an aging population.”
What About Osteoarthritis?
While the primary focus of this research has been osteoporosis, the implications extend into osteoarthritis territory as well. Osteoarthritis involves the breakdown of cartilage in joints, often compounded by the weakening of the surrounding bone structure. As researchers continue to map GPR133’s role in skeletal tissue more broadly, its influence on bone quality at joint surfaces becomes a natural next question — and one the Leipzig team is actively pursuing in follow-up projects.
Where Are We on the Road to Human Treatment?
This is where excitement must be tempered with patience though not pessimism.
As of now, human clinical trials have not yet begun. The research is at the preclinical stage, conducted entirely in mouse models. Questions about long-term safety, potential off-target effects, and human pharmacokinetics (how the body processes the drug) remain open.
However, the Leipzig team is actively pursuing follow-up projects to explore AP503 in additional disease contexts and to deepen understanding of GPR133 across different tissues. Researchers also plan to study how individuals with different GPR133 genetic variants respond to the compound, a step toward precision medicine.
A realistic clinical timeline: additional preclinical safety studies over the next two to three years, followed by Phase 1 human trials (focused on safety and dosing) potentially by the late 2020s, with efficacy trials extending beyond that. Drug development is rarely fast — but the foundation being laid here is unusually solid, with strong mechanistic understanding, clear genetic human links, and a well-funded institutional framework behind it.
Why This Discovery Matters Especially for Women
Osteoporosis is not gender-neutral. In Germany alone, approximately six million people live with the condition, the majority of them women. Globally, postmenopausal women account for the largest share of osteoporosis cases, driven by the steep drop in estrogen that accelerates bone resorption. The fact that AP503 reversed bone loss in an ovariectomy mouse model, the gold-standard preclinical simulation of postmenopausal osteoporosis, is particularly meaningful.
Current treatments like bisphosphonates (which slow bone breakdown) and parathyroid hormone analogs (which stimulate formation) have real limitations: side effects, inconvenient delivery methods, and loss of efficacy over time. A receptor-targeted therapy that works with the body’s natural sensing machinery, and that pairs synergistically with exercise, could represent a genuinely different kind of tool.
The Bigger Picture
What makes this research feel different from many “promising mouse studies” is the layered quality of the science. The GPR133 story is grounded in human genetic data, validated through multiple mouse models, connected to real molecular pathways, and already linked to muscle health — suggesting a possible dual therapeutic benefit for the increasingly recognized syndrome of combined muscle and bone loss in aging.
The body, it turns out, may already know how to build strong bones. It just needs the right signal. Scientists in Leipzig have found a way to send it.
Source: “The mechanosensitive adhesion G protein-coupled receptor 133 (GPR133/ADGRD1) enhances bone formation”
Signal Transduction and Targeted Therapy (Nature Publishing Group), 2025
For health enthusiasts, longevity seekers, and wellness explorers
What Is Functional Medicine?
Functional medicine is a systems-biology-based approach to healthcare that focuses on identifying and addressing the root causes of disease rather than managing symptoms. At its core, it treats the body as a single, interconnected web of biological systems — where a dysfunction in one area (say, gut health) may ripple outward to affect mood, immunity, hormonal balance, and metabolic function.
The field is sometimes called “Foundational Medicine,” a term that emphasizes its commitment to addressing the biological foundations of health: nutrition, sleep, stress physiology, gut microbiome integrity, hormonal balance, and environmental exposures. Practitioners spend considerable time — often an hour or more per patient visit — constructing detailed timelines of a patient’s health history, lifestyle habits, genetic predispositions, and environmental triggers.
The Institute for Functional Medicine (IFM), founded in 1991, is widely considered the primary certifying body and educational organization in the field, and it has done much to formalize and legitimize the discipline.
Why Practitioners Are Drawn to It
Physicians and clinicians who migrate toward functional medicine often describe a moment of professional disillusionment — a growing sense that the fifteen-minute appointment, the prescription pad, and the symptom-suppression model simply weren’t working for their most complex, chronically ill patients.
For many practitioners, the appeal is philosophical as much as clinical. Functional medicine restores the investigative nature of medicine, demanding that a doctor ask why a patient is inflamed, fatigued, or depressed, not merely what drug to prescribe. It integrates emerging research in areas like the microbiome, epigenetics, mitochondrial function, and nutrigenomics that conventional medical training often lags in teaching.
There is also a growing market reality: patients are arriving at practices already fluent in terms like “leaky gut,” “adrenal fatigue,” and “metabolic dysfunction.” Functional medicine practitioners can meet patients where they are.
Benefits to Patients
Patients who seek functional medicine care typically do so after years of frustration with conventional medicine, chronic conditions like fibromyalgia, autoimmune disease, irritable bowel syndrome, chronic fatigue, and hormonal imbalances that have been managed but never truly resolved.
The perceived benefits are significant. The extended consultation model allows for truly personalized care. Advanced lab testing — including comprehensive stool analysis, organic acid testing, micronutrient panels, and detailed hormonal assays — can reveal imbalances that standard bloodwork misses entirely. Patients frequently report feeling heard in ways they haven’t experienced in rushed conventional visits.
Treatment plans typically emphasize dietary intervention (often an anti-inflammatory or elimination protocol), targeted supplementation, lifestyle modifications, stress management, and, where appropriate, pharmaceutical support. Many patients experience meaningful improvements in energy, mood, cognitive clarity, and body composition — outcomes that feel transformative after years of symptomatic management.
How It Differs from Allopathic and Osteopathic Medicine
Conventional allopathic medicine (the MD model) is organized around diagnosing named diseases and matching them to evidence-based treatments, typically pharmaceutical. It excels at acute care, infectious disease, trauma, and surgical intervention. Where it struggles is with the gray zone of modern chronic disease — conditions that exist on a spectrum, develop over decades, and are deeply intertwined with lifestyle.
Osteopathic medicine (the DO model) introduced a more holistic framing over a century ago, emphasizing the interconnection of body systems and the body’s innate healing capacity. In practice, however, most modern DOs practice nearly identically to MDs, with osteopathic manipulative therapy as the primary distinguishing feature.
Functional medicine draws from both traditions while layering in nutritional biochemistry, environmental medicine, and systems biology. Where allopathic medicine might diagnose a patient with hypothyroidism and prescribe levothyroxine, a functional medicine practitioner would investigate why the thyroid is underperforming — exploring autoimmune triggers, iodine status, selenium deficiency, gut permeability, and toxic load before (or alongside) prescribing medication.
Who Can Become a Practitioner?
This is where functional medicine gets genuinely complex — and sometimes controversial.
The IFM’s flagship certification, the IFM Certified Practitioner (IFMCP) credential, is open to licensed healthcare professionals including MDs, DOs, nurse practitioners (NPs), physician assistants (PAs), registered nurses (RNs), registered dietitians (RDs), chiropractors, and naturopathic doctors (NDs). Candidates must complete the IFM’s Applied Clinical Training program, pass a written examination, and demonstrate a certain volume of clinical hours.
Notably, there is no requirement to be an MD or DO. This is intentional — and it is also a point of significant controversy. NPs and PAs who complete IFM training may practice functional medicine within their scope of practice, which varies by state. In some states, NPs have full practice authority; in others, they require physician oversight.
Beyond IFMCP, many practitioners operate under the functional medicine umbrella with certifications from organizations like the American Academy of Anti-Aging Medicine (A4M), which offers fellowship credentials to an even broader range of providers, including health coaches and wellness professionals in some programs.
The lack of a single, rigorous, universally recognized licensing board is one of the field’s most persistent vulnerabilities.
Prominent Practitioners
Several high-profile names have elevated functional medicine’s public profile considerably:
Dr. Mark Hyman, perhaps the most recognizable face of functional medicine, has written numerous bestselling books and served as Head of Strategy and Innovation at the Cleveland Clinic Center for Functional Medicine, lending institutional credibility to the field. His “Food as Medicine” framework has reached millions.
Dr. Andrew Weil, founder of the Arizona Center for Integrative Medicine, helped pioneer the broader integrative medicine movement and trained a generation of physicians who went on to embrace functional approaches.
Dr. David Perlmutter, neurologist and author of Grain Brain, applies functional principles to neurological health, emphasizing the gut-brain axis and the role of diet in conditions from Alzheimer’s to ADHD.
Dr. Terry Wahls became well known for using a nutrient-dense, mitochondria-focused dietary protocol to substantially reverse her own secondary progressive multiple sclerosis, an extraordinary personal and clinical story.
Dr. Peter Attia, while not strictly a functional medicine practitioner, operates in adjacent territory with his longevity-focused, data-driven approach to metabolic health and preventive medicine, and has enormous influence among the wellness and biohacking communities.
Criticisms of the Discipline
The criticisms are real and worth taking seriously. Conventional medicine’s primary objection is the evidence base — or the perceived lack of it. Many functional medicine interventions (specific supplement protocols, food sensitivity testing, adrenal fatigue assessments) have not been subjected to large randomized controlled trials, and critics argue that the explanatory frameworks can be pseudoscientific.
The “adrenal fatigue” diagnosis is a prime example: mainstream endocrinology does not recognize it as a condition, while functional practitioners regularly test for and treat it. Similarly, “leaky gut” as a framework is scientifically plausible and increasingly supported by research in intestinal permeability, but its application in clinical practice often runs ahead of the evidence.
Cost is another significant barrier. Functional medicine visits are frequently not covered by insurance, and the advanced lab panels, sometimes costing thousands of dollars, fall entirely out of pocket. This concentrates access among affluent, typically well-educated patients, raising equity concerns.
Controversies and Scandals
The broader integrative and functional medicine space has not been immune to controversy. The A4M and some affiliated practitioners have faced criticism for promoting anti-aging hormone therapies, including high-dose human growth hormone (HGH) and testosterone, with marketing claims that regulators have scrutinized.
Several practitioners operating under a functional medicine label have been the subject of medical board complaints for practicing beyond their training, particularly when non-physician providers undertake complex diagnostic workups or recommend aggressive supplement regimens without adequate oversight.
The supplement industry nexus is also a persistent concern. Many functional medicine practices generate substantial revenue by selling proprietary supplement lines directly to patients, creating a financial conflict of interest that critics argue compromises clinical objectivity.
And in the age of social media, “functional medicine” has become something of a branding term that virtually anyone can adopt. Health coaches and influencers with minimal clinical training can claim functional medicine expertise, blurring the line between legitimate practitioners and wellness marketers — a problem the IFM has acknowledged but struggled to fully address.
The Bottom Line
Functional medicine represents a genuine and often valuable evolution in thinking about chronic disease, one that takes seriously the interconnectedness of biology, lifestyle, environment, and genetics. At its best, it produces remarkable outcomes for patients whom conventional medicine has left behind. At its worst, it can be expensive, evidence-light, and practiced by undertrained providers chasing a wellness market.
For health and longevity enthusiasts, the savvy approach is to engage with its principles critically — embracing the emphasis on root-cause investigation, personalized nutrition, and lifestyle medicine while demanding the same rigorous self-questioning it claims to bring to biology. The best functional medicine practitioners hold those two things in productive tension.
The field continues to evolve rapidly. The Cleveland Clinic’s Center for Functional Medicine, academic integrative programs at institutions like UCSF and the University of Arizona, and growing research into the microbiome and metabolic health suggest that functional medicine’s best ideas may yet be folded into the mainstream — on better evidence.
A groundbreaking discovery two decades in the making
Every so often, a scientific breakthrough emerges that quietly reshapes what we believe is possible in medicine. For millions of women living with Human Papillomavirus (HPV), the work of Dr. Eva Ramón Gallegos may represent exactly that kind of turning point. A researcher from Oaxaca, Mexico, she has spent more than two decades pursuing a question that most of the medical world had left unanswered: could HPV actually be eliminated from the body? Her answer, delivered through years of painstaking research, is a resounding yes.
A Scientist Shaped by Curiosity and Dedication
Dr. Ramón Gallegos built her career at the intersection of biomedicine and biotechnology. She earned her undergraduate degree at the Universidad Veracruzana before deepening her expertise at Mexico’s prestigious Instituto Politécnico Nacional (IPN), where she completed a master’s degree in cytopathology and later a doctorate in chemical-biological sciences. A formative research residency at the University of Minho in Portugal expanded her horizons into molecular biotechnology and biophotonics — disciplines that would later prove central to her most celebrated work.
Since 2001, she has led the Environmental Cytopathology Laboratory at IPN’s National School of Biological Sciences in Mexico City, where she mentors graduate students while pushing the boundaries of non-invasive cancer treatment. Her specialty lies in finding gentler, smarter ways to fight disease — particularly cervical cancer linked to HPV.
Understanding the Problem: Why HPV Matters
HPV is the world’s most common sexually transmitted infection. With over 100 known strains and at least 14 linked to cancer, its reach is staggering — around 80% of women will contract some form of the virus during their lifetime. The World Health Organization identifies cervical cancer as the fourth most common cancer in women globally, and in Mexico specifically, it ranks as the second leading cause of cancer death among women.
For decades, medicine had no cure for active HPV infection. Prevention through vaccination — such as Gardasil — was the most powerful tool available. Once infected, patients could only wait, monitor, and manage. For Dr. Ramón Gallegos, that wasn’t good enough.
The Research Journey: Two Decades of Persistence
Her formal project launched in 2012 after she received a scholarship from Mexico’s national science council, CONACYT. But the intellectual groundwork had been laid years before. Her research centered on photodynamic therapy (PDT) — a technique that uses light-activated drugs to selectively destroy abnormal cells while leaving healthy tissue intact.
Photodynamic Therapy (PDT)
The process works like this: a photosensitizing agent called delta-aminolevulinic acid (5-ALA) is applied to the cervix. Over several hours, it converts into a fluorescent compound that accumulates in damaged or infected cells but clears quickly from healthy ones. Doctors then expose the area to a targeted light source. The compound absorbs the light and generates reactive oxygen molecules that destroy the compromised cells, a precise, almost elegant mechanism.
In an early phase of her research involving women across Mexico City, Oaxaca, and Veracruz, the results were already striking: HPV was eliminated in 85% of patients who had the virus without lesions, and in 85% of those who had both HPV and premalignant lesions. These figures alone would have been noteworthy. But Dr. Ramón Gallegos wasn’t finished.
The Breakthrough: 100% Eradication
In February 2019, the Instituto Politécnico Nacional announced results that caught the attention of scientists and journalists worldwide. In a refined second phase of the study — conducted with 29 women in Mexico City who received a higher concentration of 5-ALA over two sessions, 48 hours apart — HPV was completely eradicated in 100% of patients who had the virus without lesions. Among those with both HPV and premalignant lesions, 64.3% showed virus elimination. Even patients with lesions but no active HPV saw a 57.2% regression rate.
The announcement was fittingly made on February 11th — the International Day of Women and Girls in Science. The team of 18 researchers she led was itself a testament to inclusion: 14 of them were women.
Beyond HPV, the therapy also showed a remarkable secondary effect, eliminating pathogenic microorganisms like Chlamydia trachomatis (in 81% of patients) and Candida albicans (in 80%), while leaving beneficial bacteria largely intact.
What This Discovery Means
Dr. Ramón Gallegos has been careful to frame her results as a promising breakthrough rather than a definitive global cure, larger, peer-reviewed randomized controlled trials are still needed to confirm long-term efficacy and scalability. She has also spoken candidly about the systemic barriers she faced: underfunding, bureaucratic delays, and the chronic underinvestment in scientific research in Mexico.
Yet the significance of her work is hard to overstate. Conventional HPV-related treatments — surgical excisions, cryotherapy, biopsies — are invasive and can compromise cervical integrity and fertility. Photodynamic therapy is non-invasive, selective, and carries minimal side effects. If validated at scale, it could transform options available to women around the world, particularly in low- and middle-income countries where cervical cancer mortality remains devastatingly high.
“When I cure a woman, I’m going to be happy — and I was.”
— Dr. Eva Ramón Gallegos
That quiet satisfaction, earned through two decades of determined science, may one day be shared by millions.
Eva Ramón Gallegos • Instituto Politécnico Nacional • Photodynamic Therapy • HPV Research
Uterine Fibroids, Black Women, and the Fight for Dignified Care
A Comprehensive Medical and Social Overview
Imagine living for years with crushing pelvic pain, hemorrhagic menstrual bleeding, and fatigue so severe it derails your career and relationships — only to be told by medical professionals that your symptoms are exaggerated, or that what you are experiencing is simply a part of being a woman. For countless Black women in the United States and around the world, this is not a hypothetical scenario. It is a lived reality, compounded by a well-documented history of medical bias that continues to shape clinical encounters today.
Uterine fibroids — noncancerous growths in or on the uterus — are extraordinarily common, yet they remain one of the most mismanaged and underappreciated conditions in women’s health. Nowhere is that mismanagement more consequential than in the care of Black women, who are disproportionately affected by fibroids in every measurable dimension: incidence, severity, age of onset, and symptom burden. Understanding why this disparity exists, and what must change to correct it, is not merely a medical question. It is a matter of justice.
“Black women are 2 to 3 times more likely to develop uterine fibroids than white women — and they develop them younger, larger, and in greater numbers.”
What Are Uterine Fibroids?
Uterine fibroids, known medically as uterine leiomyomas or myomas, are benign (noncancerous) tumors that arise from the smooth muscle cells of the uterine wall. They are composed primarily of smooth muscle tissue and fibrous connective tissue, which gives them their dense, rubbery consistency. Despite being labeled “tumors,” fibroids are not cancerous and have an extremely low rate of malignant transformation, estimated at less than 1 in 1,000 cases.
Fibroids are classified by their location within the uterus. Intramural fibroids, the most common type, grow within the muscular wall of the uterus. Subserosal fibroids develop on the outer surface of the uterus and can become pedunculated, growing on a stalk. Submucosal fibroids grow just beneath the inner lining of the uterus (the endometrium) and tend to cause the most significant bleeding symptoms. Cervical fibroids arise in the cervical tissue, and intraligamentary fibroids develop within the broad ligaments supporting the uterus.
Their size varies enormously from tiny seedlings detectable only under a microscope to massive growths that can distend the abdomen and weigh several pounds. A single woman may carry dozens of fibroids simultaneously, or just one. Their clinical impact depends heavily on size, number, and location.
Incidence: How Common Are Fibroids?
Uterine fibroids are the most common benign gynecologic tumor in women of reproductive age. By age 50, cumulative incidence studies suggest that up to 70% of white women and over 80% of Black women will have had fibroids, though many cases go undetected because a significant proportion of women remain asymptomatic.
In the United States alone, it is estimated that 26 million women between the ages of 15 and 50 have fibroids, with approximately 15 million experiencing symptoms severe enough to require treatment. Globally, fibroids account for roughly one-third of all hysterectomies performed — making them the leading cause of that procedure in the United States.
The Racial Disparity: Why Black Women Bear a Heavier Burden
The disparity between Black and white women in fibroid burden is among the starkest racial health disparities documented in the United States. Research consistently shows:
Black women are 2 to 3 times more likely than white women to develop fibroids. They develop fibroids at younger ages often in their 20s, compared to the 30s and 40s more typical of white women. Their fibroids tend to be larger and more numerous at the time of diagnosis. They experience more severe symptoms, including heavier menstrual bleeding, greater pelvic pain, and higher rates of anemia. They are more likely to require surgical intervention and undergo hysterectomy at higher rates and younger ages. They have a longer average delay between symptom onset and diagnosis — a gap often driven by dismissal from healthcare providers.
A landmark study published in the American Journal of Obstetrics and Gynecology found that by age 35, approximately 60% of Black women had ultrasound-confirmed fibroids, compared to 40% of white women. By age 50, those figures rose to over 80% and 70% respectively. Critically, the study also found that Black women’s fibroids were more likely to cause clinically significant symptoms.
Pathophysiology: The Biology Behind Fibroids
The development of uterine fibroids is a complex, multifactorial process involving genetic, hormonal, cellular, and environmental factors. While much remains to be fully elucidated, significant progress has been made in understanding the key mechanisms.
Hormonal Drivers
Estrogen and progesterone are the primary hormonal drivers of fibroid growth. Fibroids are rarely seen before puberty, grow during the reproductive years when hormone levels are highest, and typically shrink after menopause, a pattern that strongly implicates these hormones. Fibroids express higher concentrations of estrogen receptors and progesterone receptors compared to normal uterine tissue, and both hormones stimulate cell proliferation and suppress programmed cell death (apoptosis) within fibroid tissue.
Growth factors, including epidermal growth factor (EGF), transforming growth factor-beta (TGF-β), and insulin-like growth factors (IGFs), also appear to mediate the growth-promoting effects of estrogen and progesterone within fibroid tissue.
Genetic Mutations
Most fibroids are clonal in origin, meaning each tumor arises from a single transformed cell. Somatic mutations (acquired, not inherited) in the gene MED12 are found in the majority of fibroids, affecting up to 70% of cases. Other identified mutations involve HMGA2 (a chromatin-associated protein), FH (fumarate hydratase), and COL4A5/COL4A6 genes. These mutations disrupt normal cellular regulation, leading to unchecked proliferation and the overproduction of extracellular matrix proteins.
Race, Vitamin D, and Biological Stress
Researchers have explored several biological mechanisms that may explain the higher fibroid burden in Black women. One of the most compelling involves vitamin D. Black women have significantly higher rates of vitamin D deficiency due in part to increased skin melanin reducing ultraviolet light absorption, and vitamin D has been shown to inhibit fibroid cell proliferation in laboratory studies. Lower vitamin D levels may therefore remove a protective brake on fibroid growth.
Chronic stress related to racial discrimination, often termed “weathering” or allostatic load, is another important factor. Prolonged exposure to systemic racism elevates cortisol and inflammatory cytokine levels, alters hormonal regulation, and may create a biological environment more conducive to fibroid development and growth. This is not a reflection of biological inferiority; it is a biological consequence of living under conditions of chronic social and racial stress.
Additionally, studies have examined differences in hair relaxer use, dietary patterns, and environmental chemical exposures. Some research has found associations between hair relaxer chemicals (which may contain endocrine-disrupting compounds) and fibroid risk, though causation has not been definitively established.
“The higher fibroid burden in Black women is not a reflection of biological inferiority — it is, in substantial part, a consequence of the lived experience of racism itself.”
Clinical Presentation: Recognizing Symptoms
Approximately 25 to 50 percent of women with fibroids experience symptoms significant enough to affect their quality of life. The most common and debilitating symptoms include:
Heavy menstrual bleeding (menorrhagia) is the most reported symptom. Women may soak through pads or tampons within an hour, pass large blood clots, and experience bleeding that lasts for more than seven days. Severe blood loss can cause iron-deficiency anemia, leading to fatigue, shortness of breath, and heart palpitations. Pelvic pain and pressure, from a constant sense of heaviness to severe cramping, can be both cyclical and noncyclical. Dysmenorrhea (painful menstruation) may be debilitating. Bulk-related symptoms occur when large fibroids compress adjacent structures: urinary frequency and urgency arise from bladder compression; constipation and bloating from rectal compression; and back or leg pain from pelvic nerve pressure. Reproductive impact includes infertility, recurrent pregnancy loss, and obstetric complications including preterm labor and abnormal placentation. Abdominal distention caused by large fibroids may cause a woman to appear visibly pregnant.
Diagnosis: Getting to the Truth
Accurate and timely diagnosis is critical, and it is here that systemic bias begins to create divergent outcomes for Black women.
Diagnostic Tools
Pelvic ultrasound is the first-line diagnostic tool for fibroids. Transvaginal ultrasound provides the most detailed visualization of smaller or intramural fibroids. It is widely available, non-invasive, and cost-effective. Magnetic resonance imaging (MRI) provides superior anatomical detail, particularly important for surgical planning, and can more accurately map fibroid number, size, and location. Sonohysterography (saline-infused ultrasound) improves detection of submucosal fibroids by distending the uterine cavity with saline. Hysteroscopy allows direct visualization of the uterine interior and can be used both diagnostically and therapeutically for submucosal fibroids.
The Diagnostic Delay Problem
Despite the availability of these tools, Black women face substantially longer delays between the onset of symptoms and receiving a fibroid diagnosis. Studies have documented an average diagnostic delay of over three years for Black women, a span during which fibroids continue growing and symptoms worsen. This delay is not simply a matter of access to care, though access disparities are real and significant. It is also a product of implicit bias, paternalism, and the systematic discounting of Black women’s pain.
Research has consistently shown that healthcare providers are less likely to prescribe adequate pain management to Black patients, more likely to attribute their symptoms to psychological causes, and more likely to dismiss their concerns without appropriate investigation. The result is that women who should be receiving pelvic ultrasounds are instead being told their pain is stress-related, that their bleeding is “normal,” or that they simply need to lose weight.
Prognosis: Living With Fibroids
Fibroids are not life-threatening, but their impact on quality of life can be profound. Women with symptomatic fibroids report significantly impaired physical functioning, social limitations, and emotional wellbeing. Work productivity losses due to heavy bleeding and pain, including missed workdays and reduced effectiveness,cost an estimated $4,000 to $6,000 per woman per year in the United States.
Most fibroids remain stable or grow slowly. After menopause, the majority shrink as estrogen levels decline. However, for women still in their reproductive years, the condition is often progressive without treatment. Untreated iron deficiency anemia from chronic blood loss can cause serious cardiovascular strain. Submucosal fibroids significantly reduce fertility and implantation rates. Pregnancy complications, including preterm delivery and placental abruption, are elevated in women with fibroids, particularly larger ones.
The prognosis following appropriate treatment is generally excellent, with most women experiencing substantial or complete symptom relief. The key word is “appropriate” which requires both access to care and providers who listen.
Treatment Options: A Spectrum of Possibilities
Fibroid treatment has expanded considerably in recent decades, offering women options ranging from watchful waiting to minimally invasive procedures to surgery. The ideal treatment depends on symptom severity, fibroid characteristics, reproductive goals, and patient preference, and every woman deserves a thorough, individualized conversation about her options.
Medical (Non-Surgical) Treatments
Hormonal therapies including combined oral contraceptives, progestin-only agents, and levonorgestrel-releasing intrauterine devices (IUDs) can reduce menstrual bleeding and relieve pain, though they do not shrink fibroids. GnRH agonists (gonadotropin-releasing hormone agonists) such as leuprolide suppress ovarian hormone production, causing fibroids to shrink temporarily. They are often used preoperatively to reduce fibroid size and blood loss but are not suitable for long-term use due to side effects including bone loss and menopausal symptoms. GnRH antagonists, including elagolix (Oriahnn) and relugolix (Myfembree), offer a newer approach with more rapid onset and some advantages in tolerability. They are now FDA-approved for fibroid-associated heavy menstrual bleeding. Tranexamic acid is a non-hormonal medication that reduces menstrual blood loss by stabilizing blood clots and can significantly reduce bleeding volume. Iron supplementation addresses anemia caused by chronic blood loss and is an important supportive therapy.
Minimally Invasive Procedures
Uterine fibroid embolization (UFE) is a radiological procedure in which the blood supply to fibroids is blocked by injecting small particles through a catheter inserted into the uterine arteries. Fibroids shrink significantly over months, with sustained symptom relief in approximately 85 to 90 percent of women. UFE preserves the uterus and has a shorter recovery time than surgery, though it is not typically recommended for women desiring future pregnancy. Focused ultrasound ablation uses high-intensity ultrasound waves, guided by MRI, to heat and destroy fibroid tissue. It is completely non-invasive and preserves fertility. Endometrial ablation destroys the uterine lining and can dramatically reduce bleeding, but it is only appropriate for women who do not wish to conceive and is best suited for smaller, submucosal fibroids.
Surgical Treatments
Myomectomy is the surgical removal of fibroids while preserving the uterus. It can be performed via hysteroscopy (for submucosal fibroids), laparoscopy, robotic assistance, or open abdominal surgery depending on fibroid size and location. Myomectomy is the preferred surgical option for women who wish to preserve fertility. Hysterectomy, complete removal of the uterus, is the only definitive cure for fibroids. It eliminates any possibility of fibroid recurrence and resolves all associated symptoms permanently. However, it also permanently ends fertility and carries surgical risks. Hysterectomy remains disproportionately performed in Black women with fibroids, a disparity reflecting both the greater severity of their disease at presentation and, in some cases, inadequate counseling about uterus-sparing alternatives.
“Every woman deserves a thorough, individualized conversation about her treatment options — not an assumption that hysterectomy is her only choice.”
The Medical Bias Crisis: When Pain Is Dismissed
The undertreatment of Black women’s pain is not a new phenomenon ; it is a pattern with deep historical roots and ongoing contemporary consequences. The myth that Black people have higher pain thresholds, or that their reported pain is exaggerated, has been traced to 19th-century pseudoscientific claims made by physicians who used enslaved Black bodies as medical subjects without anesthesia. These racist ideologies were never fully eradicated from medical culture; they evolved and persisted, embedded in implicit bias that continues to shape clinical decisions.
A widely cited 2016 study published in the Proceedings of the National Academy of Sciences found that medical students and residents — even those without overt prejudice — were significantly more likely to hold false beliefs about biological differences between Black and white patients (such as Black people having thicker skin or less sensitive nerve endings) and that those who held such beliefs were less likely to recommend adequate pain treatment for Black patients. This is not anecdote. It is published, peer-reviewed science demonstrating that bias translates into undertreatment.
For Black women with fibroids, this manifests in concrete, harmful ways. Their heavy bleeding is attributed to lifestyle. Their pelvic pain is called stress. Their requests for imaging are denied. Their descriptions of disability are questioned. And when they finally do receive a diagnosis, they are often offered only the most extreme intervention — hysterectomy — rather than being counseled about the full range of options their white counterparts routinely receive.
What Must Change: Building Equitable, Dignified Care
Providing equitable, dignified care to Black women with fibroids requires change at every level of the healthcare system — individual, institutional, and structural. The following evidence-based and justice-centered recommendations represent a roadmap for meaningful reform.
1. Believe Women — Unconditionally
The foundation of dignified care is the radical but simple act of believing patients. When a woman reports pain, bleeding, or functional impairment, the clinical response should be investigation, not skepticism. Pain should be documented, taken seriously, and evaluated with appropriate tools, not minimized because of assumptions rooted in race, size, or social status. Every provider must actively examine and challenge their assumptions about which patients’ reports of suffering are credible.
2. Eliminate Implicit Bias Through Training and Accountability
Medical schools, residency programs, and continuing medical education must integrate robust, evidence-based implicit bias training into their curricula. But training alone is insufficient. Hospitals and practices must implement accountability structures — tracking prescribing patterns, referral rates, and diagnostic delays by patient race and use that data to identify and address disparities. What gets measured gets managed.
3. Standardize Early Screening for High-Risk Populations
Given the earlier onset and greater severity of fibroids in Black women, professional medical societies should develop and implement screening guidelines that specifically address this population. A Black woman who presents to a primary care physician or gynecologist with heavy menstrual bleeding or pelvic pain should receive a pelvic ultrasound, period. Delays in diagnostic imaging must be treated as a quality-of-care failure, not an acceptable norm.
4. Expand Access to Uterus-Preserving Treatments
Black women are significantly more likely to end up with a hysterectomy than white women with comparable fibroid burden — not because their medical situation necessarily requires it, but because they are less frequently counseled about alternatives and less frequently referred to specialists who perform them. Providers must commit to presenting the full spectrum of treatment options, and healthcare systems must ensure that procedures like UFE, focused ultrasound, and laparoscopic myomectomy are accessible regardless of a patient’s insurance status or zip code.
5. Center Patient Autonomy and Reproductive Goals
Treatment decisions must be driven by the patient’s goals, values, and reproductive desires — not by assumptions based on race or socioeconomic status. A Black woman who wants to preserve her fertility and uterus has every right to pursue treatments that honor that goal. A Black woman who chooses hysterectomy for her own reasons has every right to that decision as well. The difference is whether the choice is hers, made with full information, versus a decision made for her without adequate counseling.
6. Invest in Research That Centers Black Women
Historically, fibroid research has underrepresented Black women despite their greater disease burden. NIH funding must be prioritized for studies that examine fibroid etiology in Black women specifically, assess the effectiveness of different treatments in Black patients, and investigate the role of social determinants — including discrimination, chronic stress, and environmental exposures — in fibroid development. The disparities cannot be understood or addressed without data that reflects them.
7. Diversify the Medical Workforce
Research consistently shows that Black patients receive better care from Black physicians — not merely because of cultural concordance, but because of different patterns of listening, communication, and clinical attention to patient-reported symptoms. Increasing the representation of Black physicians, nurses, and other healthcare professionals — particularly in obstetrics and gynecology — is both a workforce equity imperative and a patient safety strategy.
8. Empower Patients Through Education and Advocacy
Black women must be equipped with knowledge about fibroids — their symptoms, their options, and their rights as patients. Community health organizations, patient advocacy groups such as the White Dress Project, and social media platforms have already begun this work, helping women name their symptoms, document their experiences, and demand appropriate care. Healthcare systems should partner with — not co-opt — these community voices. Patients who arrive armed with information and the confidence to advocate for themselves are more likely to receive the care they deserve.
9. Reform Clinical Communication Standards
Provider-patient communication must be assessed and reformed. Scripts that embed dismissal — “some women just bleed more heavily,” “your pain tolerance might be lower,” “let’s watch and wait” without clinical justification — must be recognized for what they are: clinical failures with racial dimensions. Medical education must teach providers to communicate with humility, to invite patients’ perspectives, and to avoid language that diminishes or invalidates reported symptoms.
Conclusion: The Moral Urgency of Getting This Right
Uterine fibroids are not a mystery. We understand their biology, we have effective treatments, and we know who suffers most. What we lack is not knowledge ; it is the will to apply that knowledge equitably.
Black women in America have long been required to prove that their pain is real, that their suffering matters, and that they deserve the same standard of care as anyone else. That requirement is itself a form of harm layered on top of the physical burden of a condition that already disproportionately claims their energy, their fertility, and in severe cases, their organs.
Changing this will not happen through goodwill alone. It requires structural change in medical education, in research funding, in clinical protocols, and in the culture of medicine itself. It requires every provider who sees a Black woman in pain to ask themselves a simple question: Would I respond the same way if this patient were white?
Until the answer to that question is always “yes” — and the evidence confirms it — the work is not done.
“Black women deserve to be believed. They deserve to be heard. They deserve to receive the same quality of care on the first appointment that it may take others years and multiple providers to obtain.”
This article is intended for educational purposes. Women experiencing gynecologic symptoms should seek care from a qualified healthcare provider. If you feel your concerns are being dismissed, you have the right to seek a second opinion.